Sinus Membrane Elevation of a Complicated Sinus Septum Area with Vertical Bone Augmentation in Sever
- Dr. Nam Yoon Kim

- Jun 28, 2018
- 3 min read
Situation A 58-year-old female, No significant health history except for slight xerostomia.

Panoramic x-ray at the first visit. A complicated sinus septum was present between #25 and 26. the height of the remaining bone was about 2-3mm at #26 site. It appears that only thin cortical bone covers the root of #27 which invades into the sinus cavity.

Periapical x-ray after removal of the previous prosthesis. #27 was extracted due to severe caries. Near the root apex of #25, pneumatization of the sinus inferior wall was observed.


6 weeks after the extraction of #27. There seemed to be some remaining bone at #27 site. #26 site was planned to obtain a Class II/III fixation by passing through the mesial slope of the sinus and septum with the S-reamer.

After the initial osteotomy up to the depth just short of the final depth with initial straight drill, the last part of the osteotomy to penetrate the sinus septum was performed with the S-reamer of 3.2mm diameter with a 5mm stopper. Drilling at 1000-2000 rpm with copious irrigation is recommended for this procedure.

The S-reamer in the SCA kit was used to drill into the sinus cavity to achieve Class III CM fixation. Based on the radiographic analysis, residual bone height was expected to be 4-5mm.
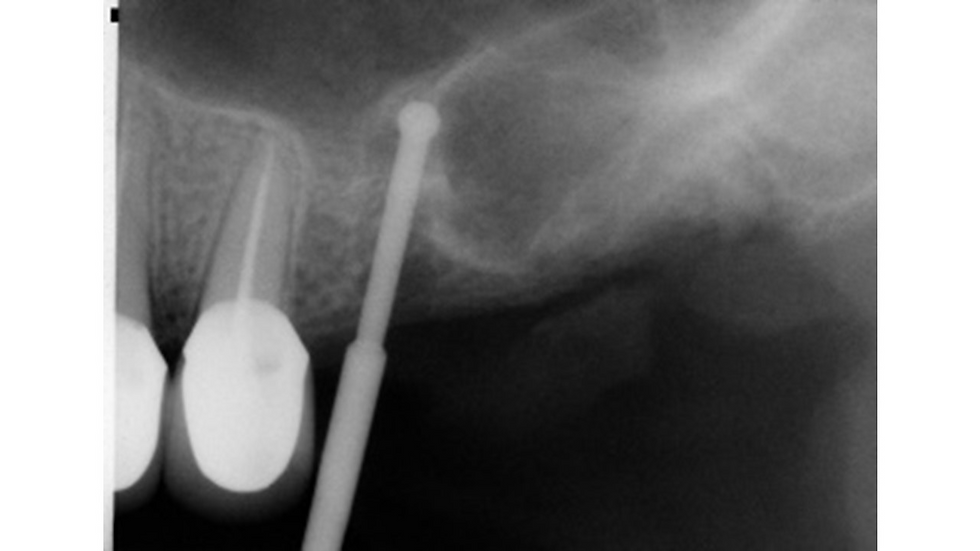
On periapical x-ray, the drilling path is shown by the depth gauge inserted into the osteotomy site. When drilling with the S-reamer, one does not perforate or tear the sinus membrane as long as the drill does not go beyond the peak of the septum. Good initial fixation can be obtained by engagement of the implant into the cortical bone of the septum.

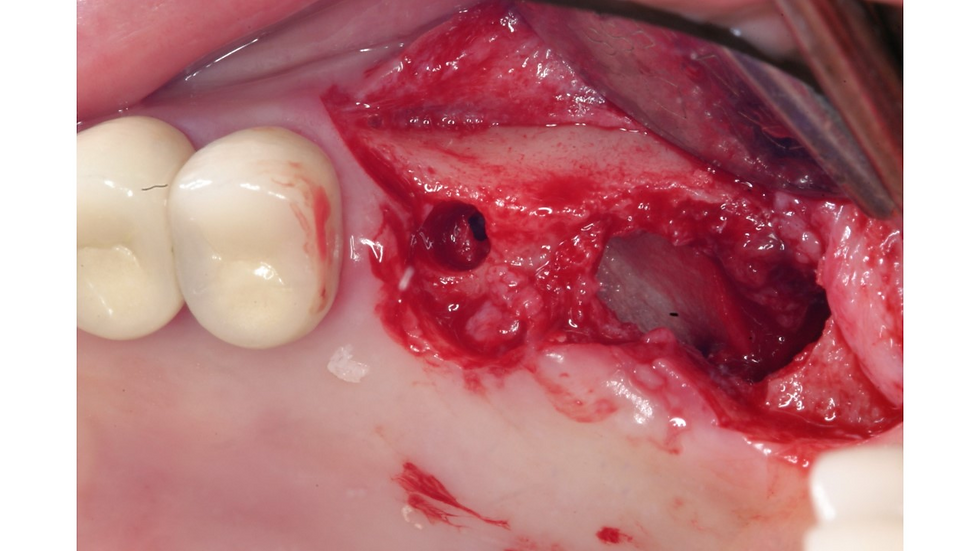
The cortical wall of the sinus septum of #26 area was eventually opened at 7mm drilling. In the #27 and 28 area a large defect was observed. The membrane fused to the soft tissue of the gingiva was cut, separated and detached from the sinus bony wall.

A collagen membrane (Lyoplant) was placed to cover the soft tissue layer, to separate the membrane from grafted bone and to prevent the downgrowth of soft tissue.
The collagen membrane cover underneath the soft layer is seen. The sinus membrane at the mesial part of the septum was detached with the S-reamer, and the membrane at the distal side of the septum was detached by the #03 elevator.

Alloplastic bone material (DM bone, Metabiomed) was inserted into the sinus cavity crestally.

The mesial side of the membrane was elevated by the S-reamer and crestal bone graft, and the rest of the sinus was elevated by the micro-elevators in the SLA kit and grafted through the large crestal opening.

A 5.0x10mm CMI EB fixture was inserted at #16 site. ITV was 40 Ncm which was probably obtained from thick inferior cortical layer engagement.


A titanium mesh (CTi-mem, E3) was adapted and placed on the grafted site. The Ti mesh was fixed by suture material. It is critical to cover CTi-mem with a collagen membrane to reduce exposure rate.

The #16 implant was non-submerged and a healing abutment was connected after implant placement. Mattress suture is usually recommended for adequate eversion of the flap.
In this case, simple interrupted and modified mattress sutures were done due to the thick gingiva.

Panoramic x-ray after surgery. The distinct outline of the grafted bone is visible. The #26 implant was loaded in 3 months by a provisional crown

6 months after surgery. Soft tissue is healed without any Ti mesh exposure.

At the time of the Ti mesh removal, the mesh was well adopted and there was no sign of infection. The volume of the grafted bone was maintained.

The removal of the CTi-mem is easier than other Titanium meshes. Underneath the Ti mesh, a solid bone mass was observed.

A 5.0X10mm CMI IS-II active fixture was placed 1mm subcrestally in the grafted bone only. The bone density and ITV were D333 and 20 Ncm.

Panoramic x-ray after the placement of implant #27. The delivery of the final prosthesis is scheduled four months after implant placement.

Occlusal view (4 months post-op): Adequate amount of attached gingiva is present around #26, but not on the buccal aspect of #27.

Upon light biting, a piece of shimstock should loosely pass through the two opposing occlusal surfaces. Heavy biting, however, should hold the shimstock between upper and lower teeth.

Panoramic x-ray after the delivery of final prosthesis.

Panoramic x-ray (5 year follow-up): No marginal bone loss is observed around implants, specially in the #27 grafted area.



Comments