Simultaneous Implant Placement with C-reamer and Full Thickness Flap: 5 Year Follow-up
- Dr. Jongyub Kim

- May 31, 2018
- 3 min read
Patient information A 67-year-old female, medically healthy and had limited masticatory ability due to missing posterior teeth in the maxilla.
Preoperative observation

Lateral view of the maxillary left edentulous ridge before surgery. Vertical space is adequate but lateral deficiency on the buccal side of the edentulous ridge is shown.

On the occlusal view, the lateral deficiency can be better visualized.

Panoramic x-ray: Multiple septa are seen in both right and left sinuses. Due to the amount of bone graft required, crestal approach for the anterior part and lateral approach for the posterior part of the sinus are preferred. In the posterior region, the number of implants required should match the number of missing teeth.

After the flap is reflected, it turned out the buccal bony deficiency did not require advanced buccal bone augmentation.
The dark shadow shown on the buccal side implies the lateral wall of the sinus is very thin.

The C-reamer was used for lateral sinus graft. Drilling with 2000 rpm or faster is recommended for the C-reamer.

A dark shadow is seen under the outline of the C-reamer.
During window preparation with the C-reamer, the reamer should not touch the sinus membrane directly. To avoid membrane perforation, osteotomy should not be performed in full depth and the bone core should be removed by green stick fracture. When the shadow becomes darker, it implies that the reamer is getting closer to the membrane(Left). The cut-out bone core is detached from the membrane by an explorer after fracture by tapping (Right).

Note the bone core is very thin and the sinus membrane is now visible through the window. This membrane was detached by a mushroom elevator all around the window hole but it can tear the membrane if the sinus wall has an irregular or sharp surface, or septum. In that case, the other #01micro-elevator should be used.

A #03 elevator is used to detach sinus membrane meticulously. A septum is seen after detaching the sinus membrane. Small size elevators are convenient in a case like this (Left). The membrane is completely detached and lifted away from the bone (Right).

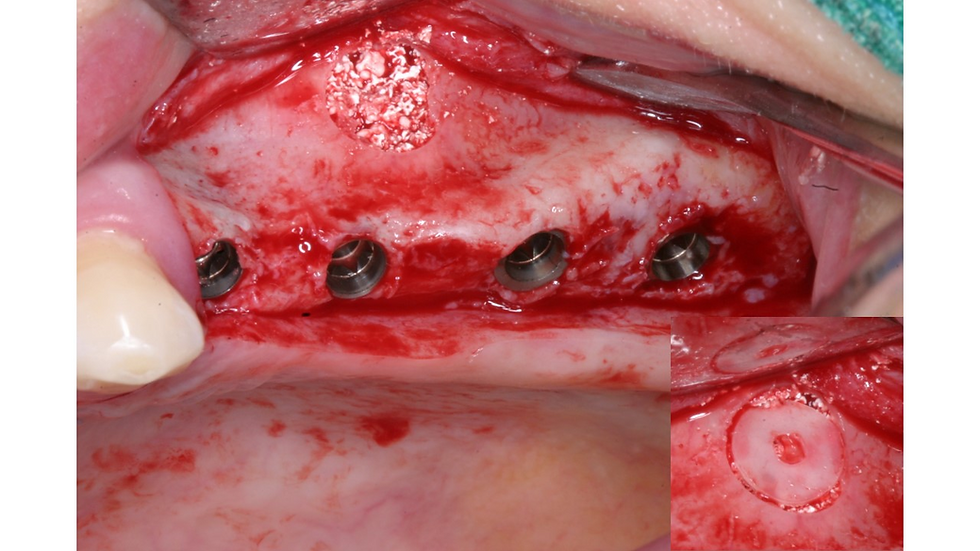
A genograft (DM bone, Metebiomed, Korea) was used for the sinus. After bone grafting, 4 implants (CMI IS-II active, Neobiotech, Korea) were placed simulteneously. Approximately 40 Ncm of insertion torque was obtained for each implant, even in the area of 2-3mm available bone. A bone core was repositioned without any fixation. Bone healing is better and faster with the repositioned bone core, which is one of the advantages of the C-reamer. The lateral and lingual bone of #25 was augmented by autogenous bone harvested from the tuberosity mixed with an allogenic bone (RegenOss, Cellumed, Seoul, Korea).
A genograft (DM bone, Metebiomed, Korea) was used for the sinus. After bone grafting, 4 implants (CMI IS-II active, Neobiotech, Korea) were placed simulteneously. Approximately 40 Ncm of insertion torque was obtained for each implant, even in the area of 2-3mm available bone. A bone core was repositioned without any fixation. Bone healing is better and faster with the repositioned bone core, which is one of the advantages of the C-reamer. The lateral and lingual bone of #25 was augmented by autogenous bone harvested from the tuberosity mixed with an allogenic bone (RegenOss, Cellumed, Seoul, Korea).

Healing abutments were connected and simple interrupted sutures were made in between healing abutments.

Panoramic x-ray after sinus graft and placement of implants.

Soft tissue healing is completed after 2 months. Sufficient keratinized gingiva is created on the buccal aspect of the ridge.
A 4-unit PFM FPD (SCRP) was delivered 4 months after implant placement.

Buccal view of the final prostheses.
2 year follow-up on the final prosthesis.

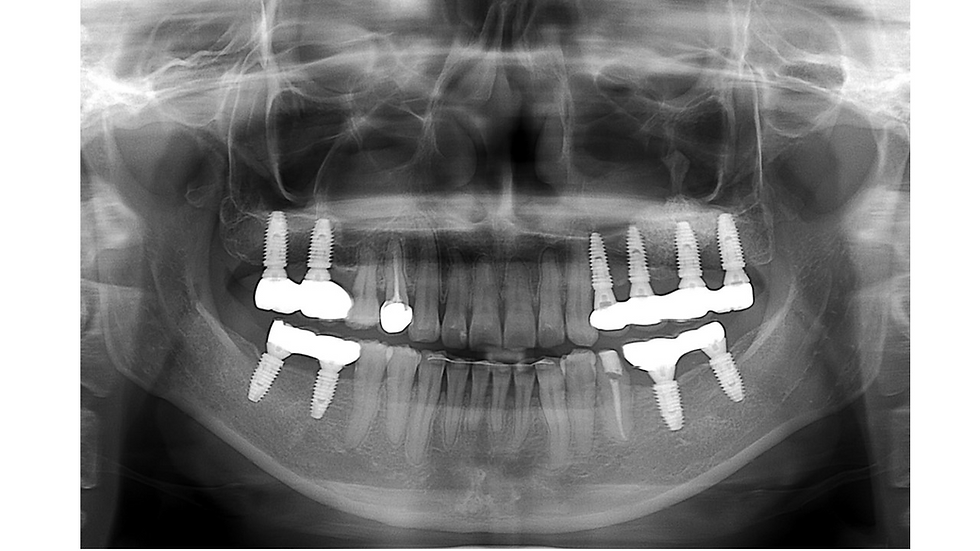
Panoramic x-ray (5 year follow-up).

Periapical x-ray after 5 years. Minimal bone loss around implants is observed.



Comments