Management of a Severely Resorbed Ridge using ALX Implant
- GAO
- Sep 10, 2025
- 3 min read

Updated: Sep 10, 2025

Case Summary 🔎
Patient Information
Past Medical History: History of Diabetes under medication
Drug allergy: None
Introduction
The patient presented with missing at #43 due to implant failure and severe mobility with inflammation at #42 and #45. Teeth #42 and #45 were extracted, and after a 3-month healing period, GBR was performed to augment the ridge. However, postoperative inflammation developed, resulting in failure of graft osseointegration and necessitating an additional bone graft. At 5 months after GBR, a 6 mm short ALX implant was subsequently placed without simultaneous GBR. The implant achieved primary stability without additional grafting, impressions were taken at 4 months, and the definitive prosthesis was delivered 5 months after implant placement. At the 3-month follow-up, the restoration remained stable without complications.
Treatment Plan
Extraction of #42,45
GBR at the mandibular anterior site (#42-45)
Implant placement at #43,45 with ALX
Digital impression
Final restoration with Zirconia crown
3-month follow up
Case Presentation
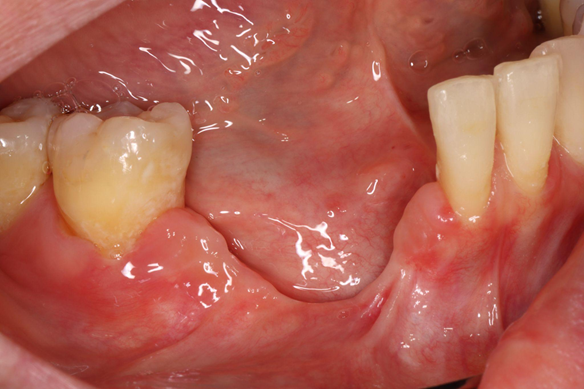
1️⃣ Pre-Op



2️⃣ Surgery - ALX Implant Placement
Autogenous bone harvesting performed using a Ø6.0 ACM.
Autogenous bone was mixed with allogenic and synthetic graft materials.
Bone graft material inserted into the defect area under the flap.
Suturing of the incision site.










Panoramic radiograph and intraoral photograph after Bone graft at the mandibular anterior site.




At 4 months post-GBR, the grafted site showed failure with insufficient bone volume formation.




Incision for tunneling technique performed in preparation for additional GBR.




Placement of bone graft material composed of synthetic graft and PDRN (polydeoxyribonucleotide).




Post operative intraoral photograph and panorama




Intraoral photograph and panoramic radiograph at 4 months post-GBR.










Maxy was performed at #45 due to dense areas within the grafted bone.




Careful removal of the implant from the ampoule.
An ALX-IT 5.5 × 6 mm, Cuff 3 mm was placed at #45, achieving 40N/cm of insertion torque.












Bone grafting performed with a mixture of synthetic bone and PDRN.
The grafted site was covered with a resorbable membrane.




Postoperative view showing primary closure with sutures.
Post-operative panoramic radiograph






3️⃣ Post-Op
At 4 months postoperatively, well healed soft tissue and regenerated bone were observed.




After uncovery, impressions were taken, followed by connection of healing abutments.




Connection of 3 mm healing abutments and measurement with AnyCheck.
At #43, IST value was 79. With an ALX cuff height of 4 mm and a 3 mm healing abutment (+6 adjustment), the corrected IST was 85.
At #45, the IST value was 81. With an ALX cuff height of 3 mm and a 3 mm healing abutment (+4 adjustment), the corrected IST was also 85.

After uncovery, impressions were taken, followed by connection of healing abutments.
4️⃣ Final Restoration
1 month later, soft tissue healing was achieved and the definitive prosthesis was fabricated




The definitive prosthesis was delivered.




Intraoral and extraoral photographs after delivery of the final restoration.





5️⃣ Follow-Up
Clinical photograph and PA radiograph at 3-month follow-up showing well-maintained prosthetic stability.






💡Conclusion
This clinical case demonstrates the successful rehabilitation of the mandibular anterior region using short ALX implants following implant failure and ridge resorption. Initial challenges, including failed osseointegration after GBR and severe bone loss, were effectively managed through a staged surgical approach involving autogenous and synthetic grafting materials, as well as PDRN application.
Despite complications after the initial grafting, subsequent bone augmentation and careful implant placement using short-length implants achieved favorable primary stability and osseointegration. The use of digital impressions facilitated precise prosthetic fabrication, and the final zirconia restoration exhibited excellent soft tissue adaptation and esthetic integration.
At the 3-month follow-up, the implants and prosthesis remained stable with no signs of inflammation or mechanical complications, suggesting that even in compromised anatomical sites, predictable outcomes can be achieved through meticulous planning, appropriate biomaterial selection, and careful surgical execution.



Comments